Virtual reality
The introduction of virtual reality to the field of neurorehabilitation has given rise to new tools for the
assessment and rehabilitation of cognitive impairments that were designed to overcome the limitations of
traditional tests and interventions. Virtual reality systems can recreate safe, ecological, and
individualized 3D environments where individuals are required to perform specific actions to achieve a goal.
As an assessment tool, virtual reality can register and objectively measure the performance of individuals
within the virtual world and their behavioral responses. Virtual street-crossing systems are particularly
interesting because they provide therapists with ecological and behavioral data for the evaluation of
extrapersonal neglect and patient autonomy in the outdoor environment. They also allow for the recreation of
a potentially hazardous real-life situation, which cannot otherwise be trained. Street crossing involves
intact attentional, perceptual and executive skills to evaluate whether traffic conditions guarantee the
safe performance of the task.
We developed a virtual reality street-crossing system that consisted of a standard computer, an audio-visual
output system, an infrared tracking system TrackIR 4:PRO (NaturalPoint Inc., Corvallis, OR), and a
joystick.1 The tracking system consists of an
infrared camera, which was attached to the upper side of the screen, and a clip with a constellation of
three reflective marks, which was mounted on a cap. Only the yaw angle was transferred to the virtual world
to represent the rotation of the head when exploring the traffic conditions of the roads. Navigation within
the virtual environment was enabled by the joystick. The system allowed subjects to walk (forward, backward,
left, and right), stop, and turn. The virtual system recreates a real street intersection with a central
roundabout that can be customized with traffic lights, litter baskets, and sound distractors, such as
ambulance sirens. The interactive area of the virtual environment consists of a crosswalk that intersects
two two-way roads with median strips that lead to the roundabout. The virtual world is presented using a
first-person view. A random number of cars drive through the roads and behave in accordance with the traffic
conditions.
To determine the convergent validation of the virtual reality system with standardized clinical tests we enrolled healthy subjects, and individuals with stroke with and without neglect.2 All the participants underwent two consecutive sessions, where they were asked to move from the starting point to a large department store and then to come back as quickly and safely as possible.
Healthy subjects completed the task more quickly and safely than individuals with stroke. From these,
individuals without neglect finished the task more quickly and safely than participants with neglect.
Individuals with stroke without neglect looked to the left and to the right side of the road more often than
participants with neglect or healthy subjects. For stroke participants without neglect, the number of left
turns was higher than the number of right turns. The time to complete the task significantly correlated with
all timed tests (Conner’s Continuous Performance Test-II, Color Trail Test, and Behavioral Assessment of the
Dysexecutive Syndrome) and with the number of errors on the Continuous Performance Test and the raw scores
on the Behavioral Assessment of the Dysexecutive Syndrome tests. The number of head turns to the left and
right significantly correlated with the Stroop Test, and the number of left head turns also correlated with
the Rivermead Behavioural Inattention Test. The outcomes of the virtual reality system, the scores of the
neuropsychological tests, and the correlations between them confirmed the reliability and convergent
validity of the street-crossing system. Its low-cost could also facilitate its integration and use in the
clinical setting.


Eye tracking
To explore the potential of this technology for assessing unilateral spatial neglect in stroke survivors we
performed a pilot study with a 65-year-old woman with an ischemic focal lesion in the non-dominant cerebral
hemisphere who was admitted to our facility.3
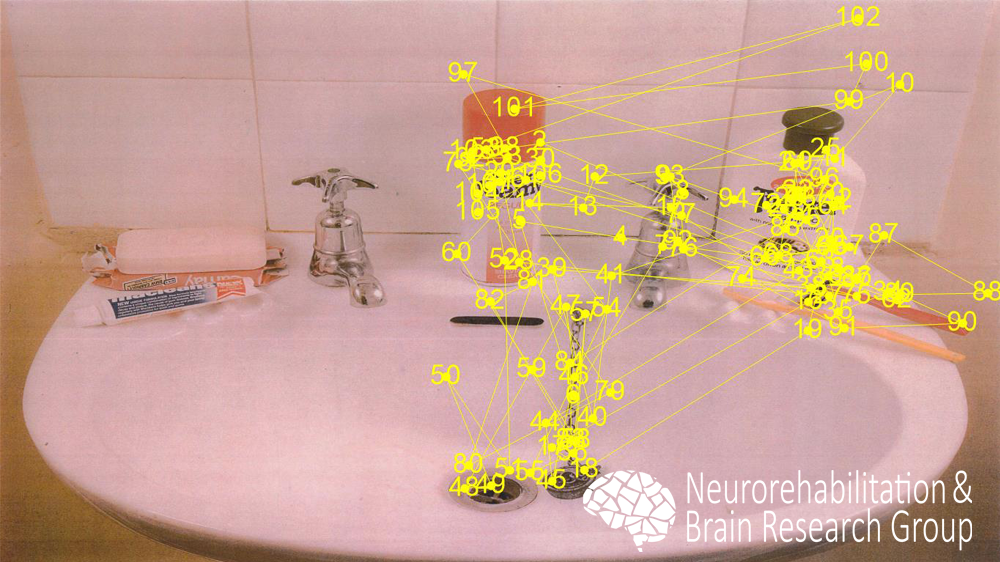
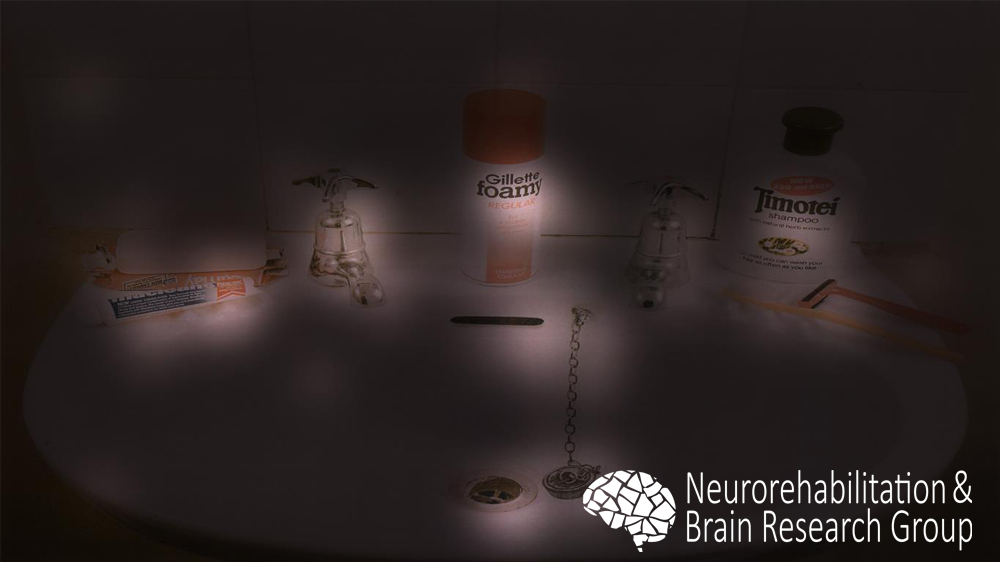
Symptomatology included severe left hemiparesis and pronounced unilateral spatial neglect syndrome. The
woman and a healthy age-matched woman were enrolled in an eye tracking study where they were required to
look for 60 seconds an image of the Behavioral Inattention Test and name the items present in it. Gaze
parameters of both subjects were recorded and heat maps were estimated as superimposed distributions of eye
fixations. In contrast to the healthy subject (see left column), who revealed distributed fixations in all
the image, the stroke survivor presented an absence of fixations in the left side of the image (see right
column), thus confirming the diagnosis and illustrating the behavioral complications that affected her
everyday functioning.
Benefits of this protocol could be threefold: first, it provides qualitative (visual) but also quantitative (fixation times, gaze patterns, etc.) information; second, it is easy to administer and not time-consuming; and third, no specific cognitive or psycholinguistic condition is required to patients. In addition, low-cost eye-tracking devices are available for $100. Even though these results are preliminary and the study focuses on the visual input and the peripersonal space, it could be a potential tool to provide relevant information about the deficits and their functional consequences.
References
- Llorens R., Navarro M.D., Alcañiz M., Colomer C., Noé E. Convergent validation of a virtual reality-based street crossing with neuropsychological tests in neglected and non-neglected stroke patients. 9th Intl Conf. Disability, Virtual Reality & Associated Technologies, 2012. 467-470.
- Navarro M.D., Llorens R., Noé E., Ferri J., Alcañiz M. Validation of a low-cost virtual reality system for training street-crossing. A comparative study in healthy, neglected and non-neglected stroke individuals. Neuropsychological Rehabilitation, 2013. 23(4): 597-618.
- Llorens R., Noé E. Through the eyes of neglect patients. The Journal of Neuropsychiatry & Clinical Neurosciences, 2015. 28(1): e8-e9.